As part of the STREAM workshop series, Dr. Jeremy Howick gave a seminar on March 25th on the usefulness of basic science research. This a great question to ask, and in his answer he makes two valid observations: 1) there’s a 70/30 split in research funding favoring basic science over clinical research and 2) historically, we have had more scientific advances accidentally than through the current system of finding a protein, characterizing its metabolic pathway, and developing and testing a drug that takes advantage of it. The best example is aspirin – we used salicylic acid for centuries before figuring out how it works.
Dr. Howick argues that we should test the wealth of information we already have – urban legends, homemade flu remedies, medicinal herbs – in more trials, and depend less on basic science research’s ability to develop drugs that we may (read: probably cannot) end up using. He argues that this is something of a win-win situation. For example, consider the case of chicken soup: Grandmothers are under the impression that it cures colds. If we test its efficacy in trials and it really works, we can figure out how, and perhaps develop a drug that is more effective. Whereas if the soup fails to cure colds, we can then definitively disprove its effectiveness, saving a lot of people, a lot of money in the canned-goods aisle.
Given the billions of dollars wasted each year in drug development, this seems a promising proposal. The presentation sparked an hour-and-a-half-long debate, however, probably because it was given to a room full of people with basic-science backgrounds. Although I agree with Dr. Howick on a lot of points, I don’t think using observational data to generate hypotheses is quite the panacea he makes it out to be. Sometimes testing folk remedies actually ends up creating more confusion. Take, for example, vitamin C: despite the dozens of clinical trials disproving its ability to cure the common cold, I’ve seen people (pharmacology students) swear up and down that it is the best cold remedy ever bottled. This just shows how pseudoscience (I’m looking at you, homeopathy) can be incredibly difficult to disprove.
@Manual{stream2015-766,
title = {So How Useful is Basic Science Research?},
journal = {STREAM research},
author = {Yasmina Hachem},
address = {Montreal, Canada},
date = 2015,
month = apr,
day = 17,
url = {http://www.translationalethics.com/2015/04/17/so-how-useful-is-basic-science-research/}
}
MLA
Yasmina Hachem. "So How Useful is Basic Science Research?" Web blog post. STREAM research. 17 Apr 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/04/17/so-how-useful-is-basic-science-research/>
APA
Yasmina Hachem. (2015, Apr 17). So How Useful is Basic Science Research? [Web log post]. Retrieved from http://www.translationalethics.com/2015/04/17/so-how-useful-is-basic-science-research/
For the first time, STREAM will be co-hosting a workshop event with CIRST, the Centre interuniversitaire de recherche sur la science et al technologie.
On April 9th at UQAM (see full location info below), Kristin Voigt will be speaking on “E-cigarettes and Smoking Norms: Do Concerns About the Renormalisation of Smoking Justify Regulation of E-cigarettes?” All are welcome, so please join us!
Dr. Voigt received her DPhil in political philosophy from the University of Oxford and has held post-doctoral positions at McGill, Harvard, Lancaster University and the European College of Liberal Arts. Her research focuses on egalitarian theories of distributive justice and the links between philosophy and social policy. Her recent and ongoing projects address issues such as conceptions and measures of health and health inequality; the use of incentives to improve health outcomes; (childhood) obesity; higher education policy; and smoking and tobacco control.
Thursday, April 9, 2015 3:00 – 5:00 PM UQAM, 1205 rue Saint-Denis, Pavillon Paul-Gerin-Lajoie, Room N-8510
@Manual{stream2015-755,
title = {Kristin Voigt, co-hosted by STREAM and CIRST},
journal = {STREAM research},
author = {STREAM admin},
address = {Montreal, Canada},
date = 2015,
month = apr,
day = 2,
url = {http://www.translationalethics.com/2015/04/02/kristin-voigt-co-hosted-by-stream-and-cirst/}
}
MLA
STREAM admin. "Kristin Voigt, co-hosted by STREAM and CIRST" Web blog post. STREAM research. 02 Apr 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/04/02/kristin-voigt-co-hosted-by-stream-and-cirst/>
APA
STREAM admin. (2015, Apr 02). Kristin Voigt, co-hosted by STREAM and CIRST [Web log post]. Retrieved from http://www.translationalethics.com/2015/04/02/kristin-voigt-co-hosted-by-stream-and-cirst/
Jeremy Howick’s research draws on his interdisciplinary training as a philosopher of science and clinical epidemiologist. He has two related areas of interest: (1) Evidence-Based Medicine (EBM), including EBM ‘hierarchies’ of evidence, clinical epidemiology, and how point of care tests might improve practice; and (2) philosophy of medicine, including the epistemological foundations of Evidence-Based Medicine, and the ethics of placebos in trials and practice.
On March 25th at 3 PM, he will be speaking on “How Useful is Basic Mechanistic Research for Discovering Medical Treatments that Benefit Humans?” All are welcome, so please join us!
@Manual{stream2015-725,
title = {Jeremy Howick visits STREAM on March 25th},
journal = {STREAM research},
author = {STREAM admin},
address = {Montreal, Canada},
date = 2015,
month = mar,
day = 11,
url = {http://www.translationalethics.com/2015/03/11/jeremy-howick-visits-stream-on-march-25th/}
}
MLA
STREAM admin. "Jeremy Howick visits STREAM on March 25th" Web blog post. STREAM research. 11 Mar 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/03/11/jeremy-howick-visits-stream-on-march-25th/>
APA
STREAM admin. (2015, Mar 11). Jeremy Howick visits STREAM on March 25th [Web log post]. Retrieved from http://www.translationalethics.com/2015/03/11/jeremy-howick-visits-stream-on-march-25th/
On 2015 February 18, James Overton visited the STREAM research group in Montreal, where he presented his research into what scientists are doing when give an explanation for something. Many accounts of scientific explanation have been offered by philosophers of science over the years, but Overton’s offering differs in that he set out to establish his account of scientific explanation by actually examining the scentific literature. Specifically, he took a year’s worth of papers from the journal Science, converted them to unformatted text, and then parsed them using the Python Natural Language Toolkit.
Overton’s methods were an analysis of word frequencies and a random sampling of sentences that seem to be making explanations, to see what sorts of data are used to justify what other sorts of claims. The most shocking result, at least for me, was that the word “law” was almost never used in the sample that Dr Overton described. That’s not to say that there is no discussion of natural laws at all, but given how much space the description of laws takes up in most accounts of scientific explanation, this seemed to be a very striking finding at the least.
This technique is very versatile and could be applied to a number of projects, from exploring the nature of scientific explanation, as Dr Overton has done, or even to a more simple project analysing the frequency of phrases like “sorafenib showed a modest effect,” or “adverse events were manageable,” and seeing if there is any relationship between the word chosen and the result being described.
@Manual{stream2015-716,
title = {Semantic natural language processing and philosophy of science},
journal = {STREAM research},
author = {Benjamin Gregory Carlisle},
address = {Montreal, Canada},
date = 2015,
month = mar,
day = 5,
url = {http://www.translationalethics.com/2015/03/05/semantic-natural-language-processing-and-philosophy-of-science/}
}
MLA
Benjamin Gregory Carlisle. "Semantic natural language processing and philosophy of science" Web blog post. STREAM research. 05 Mar 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/03/05/semantic-natural-language-processing-and-philosophy-of-science/>
APA
Benjamin Gregory Carlisle. (2015, Mar 05). Semantic natural language processing and philosophy of science [Web log post]. Retrieved from http://www.translationalethics.com/2015/03/05/semantic-natural-language-processing-and-philosophy-of-science/
James Overton is the founder of Knocean, a consulting and development service at the intersection of philosophy, science, and software. Example projects include ontology development and deployment, building semantic web tools, and developing custom web applications for scientific and medical projects. He specializes in scientific database integration using biomedical ontologies.
On February 18th at 3 PM, he will be speaking on “Explanation in Science“. All are welcome, so please join us!
@Manual{stream2015-701,
title = {James Overton visits STREAM on February 18th},
journal = {STREAM research},
author = {STREAM admin},
address = {Montreal, Canada},
date = 2015,
month = feb,
day = 11,
url = {http://www.translationalethics.com/2015/02/11/james-overton-visit-stream-on-february-18th/}
}
MLA
STREAM admin. "James Overton visits STREAM on February 18th" Web blog post. STREAM research. 11 Feb 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/02/11/james-overton-visit-stream-on-february-18th/>
APA
STREAM admin. (2015, Feb 11). James Overton visits STREAM on February 18th [Web log post]. Retrieved from http://www.translationalethics.com/2015/02/11/james-overton-visit-stream-on-february-18th/
Last year, Jonathan and I published a critique of unequal allocation ratios in late-phase trials. In these trials, patient-subjects are randomly allocated among the treatment arms in unequal proportions, such as 2:1 or 3:1, rather than the traditional equal (1:1) proportion. Strangely, despite introducing an additional burden (i.e., requiring larger sample sizes) the practice of unequal allocation is often defended as being “more ethical”. In that piece, published in Neurology, we showed that these purported ethical advantages did not stand up to careful scrutiny.
In a new article at Clinical Trials, Jonathan and I extend this line of argument to trials that use outcome-adaptive allocation. In an outcome-adaptive trial, the allocation ratio is dynamically adjusted over the course of the study, becoming increasingly weighted toward the better-performing arm. In contrast to the fixed but unequal ratios described above, outcome-adaptive ratios can sometimes reduce the necessary sample size to answer the study question. However, this reduction in cost and patient burden is not guaranteed. In fact, it only occurs when the difference between the observed effect sizes is large. And since there is no way to know in advance what this difference is going to be, these potential gains in efficiency due to outcome-adaptive designs are something of a gamble.
Nevertheless, just as we saw with fixed unequal ratios, proponents of outcome-adaptive trials claim that this allocation scheme is “more ethical”. Setting aside the sample size issue, they argue that outcome-adaptive trials better accommodate clinical equipoise by collapsing the distinction between research and care. As it is sometimes put rhetorically: Would you rather be the last subject treated in a trial or the first subject treated in practice? The outcome-adaptive trial dissolves any ethical tension in this question. The treatment will be the same either way.
Of course, any long-time readers of this blog will recognize a misunderstanding of clinical equipoise embodied in that question. The salient issue is not a comparison between the last subject enrolled in a study and the first patient treated in the context of clinical care. Rather, it is about ensuring that no subject is systematically disadvantaged by participating in a trial (and that all participants receive competent medical care). In which case, the relevant rhetorical question needs to be re-phrased as follows: Would you rather be the first patient enrolled in a study or the last? In a traditional 1:1 RCT design, clinical equipoise dissolves the ethical tension in that question. But for an outcome-adaptive design, you should hope to be the last–and that is a serious problem.
@Manual{stream2015-693,
title = {Nope– It’s Still Not Ethical},
journal = {STREAM research},
author = {Spencer Phillips Hey},
address = {Montreal, Canada},
date = 2015,
month = feb,
day = 10,
url = {http://www.translationalethics.com/2015/02/10/nope-its-still-not-ethical/}
}
MLA
Spencer Phillips Hey. "Nope– It’s Still Not Ethical" Web blog post. STREAM research. 10 Feb 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/02/10/nope-its-still-not-ethical/>
APA
Spencer Phillips Hey. (2015, Feb 10). Nope– It’s Still Not Ethical [Web log post]. Retrieved from http://www.translationalethics.com/2015/02/10/nope-its-still-not-ethical/
Every year in Canada around 50,000 people suffer brain injuries, with those experiencing severe traumas often becoming comatose for days or weeks post-incident. While there exists a battery of physiological prognostic indicators, such as pupillary light reflex (or lack thereof), and patterns of EEG activity, there remains a significant subset of patients who retain an indeterminate prognosis even after their completion. The use of sophisticated imaging techniques like fMRI has provided a modern way of mapping residual cognitive function in newly comatose patients. Currently, three fMRI studies have looked at the preservation of neural connectivity of two brain networks as potential markers of outcome. While all these studies found a (modest) positive correlation between the BOLD signal strength of the intact network and better patient outcome, significant further work is required before the technique could become clinically useful.
Dr. Charles Weijer of Western University, stresses, however, that this imminent research raises several ethical concerns: patients do not have decisional capacity, time restraints may not permit the proper procurement of surrogate informed consent, critically ill patients are clearly a vulnerable population, and it is not clear how the fMRI study results would impact patient prognosis and treatment decisions. As well, there exist practical concerns including the intra-hospital transport of patients to the fMRI machine, and the time needed outside of the ICU to perform the scans.
As a recent graduate in neuroscience another particular concern struck me – why had the researchers of the previous fMRI studies only considered two networks? The first mapped the preservation of activity in S1 after a stimulus to the hand, while the following two studies assessed the resting state connectivity of the default mode network. These are just two of several networks that have been mapped and are reliably found in healthy patients. I would be curious to see if there is prognostic contribution by analyzing other connectivity, like the auditory or executive resting state networks. Exploring the integrity of several neural networks as potential prognostic indices may allow future research to hone in on a target rather than just testing on a ‘one by one’ basis.
An analogous issue has emerged at STREAM regarding the trajectory of research in the field of cancer biomarkers and the proper method of exploring a new study space. Similar to the intended use of fMRI in previous situation, the biomarkers are being evaluated as predictive markers of outcome to specific cancer therapies. We have noticed that early studies in this field apply a very narrow set of research techniques to try and validate a biomarker. These methods are often suboptimal and it is only much later down the road that researchers branch out into other more successful methods. A notable example of this is can be seen in our evaluation of the research trajectory of one potential biomarker in lung cancer – ERCC1. A non-specific antibody had been routinely used to detect the presence of the marker, and it wasn’t until years later that basic research into a more appropriate antibody was initiated. This is likely part of the reason for the notably sluggish progress in the field. We propose that ideally, novel research programs would start with studies looking at a broad set of potential targets and then taper these down over time, as the accumulating evidence would warrant. Acutely comatose patients are a new and important population for fMRI studies, and to me it seems like this research program might benefit by encouraging future studies to evaluate and compare the predictive use of multiple networks so that they most rigorously map the study space.
Context: On January 12th, Charles Weijer, visiting from the Rotman Institute of Philosophy at Western University, gave the first talk in the new STREAM speaker series. He spoke on the ethical considerations involved in performing fMRI studies on acutely comatose patients in the ICU.
@Manual{stream2015-683,
title = {Charting the Unpredictable: Using fMRI patterns to determine outcome in acutely comatose patients},
journal = {STREAM research},
author = {Brianna Barsanti-Innes},
address = {Montreal, Canada},
date = 2015,
month = feb,
day = 6,
url = {http://www.translationalethics.com/2015/02/06/charting-the-unpredictable-using-fmri-patterns-to-determine-outcome-in-acutely-comatose-patients/}
}
MLA
Brianna Barsanti-Innes. "Charting the Unpredictable: Using fMRI patterns to determine outcome in acutely comatose patients" Web blog post. STREAM research. 06 Feb 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/02/06/charting-the-unpredictable-using-fmri-patterns-to-determine-outcome-in-acutely-comatose-patients/>
APA
Brianna Barsanti-Innes. (2015, Feb 06). Charting the Unpredictable: Using fMRI patterns to determine outcome in acutely comatose patients [Web log post]. Retrieved from http://www.translationalethics.com/2015/02/06/charting-the-unpredictable-using-fmri-patterns-to-determine-outcome-in-acutely-comatose-patients/
Charles Weijer is a philosopher, physician, and the Canada Research Chair in Bioethics at Western University. His academic interests center on the ethics of medical research. He has written about using placebos in clinical trials, weighing the benefits and harms of medical research, and protecting communities in research.
On January 12th at 3 PM, he will be speaking on “Ethical Considerations in Functional MRI Studies on Acutely Comatose Patients in the Intensive Care Unit”. All are welcome, so please join us!
@Manual{stream2015-673,
title = {Charles Weijer visits STREAM on January 12th},
journal = {STREAM research},
author = {STREAM admin},
address = {Montreal, Canada},
date = 2015,
month = jan,
day = 5,
url = {http://www.translationalethics.com/2015/01/05/stream-workshop-series-january-15th-charles-weijer/}
}
MLA
STREAM admin. "Charles Weijer visits STREAM on January 12th" Web blog post. STREAM research. 05 Jan 2015. Web. 26 Apr 2025. <http://www.translationalethics.com/2015/01/05/stream-workshop-series-january-15th-charles-weijer/>
APA
STREAM admin. (2015, Jan 05). Charles Weijer visits STREAM on January 12th [Web log post]. Retrieved from http://www.translationalethics.com/2015/01/05/stream-workshop-series-january-15th-charles-weijer/
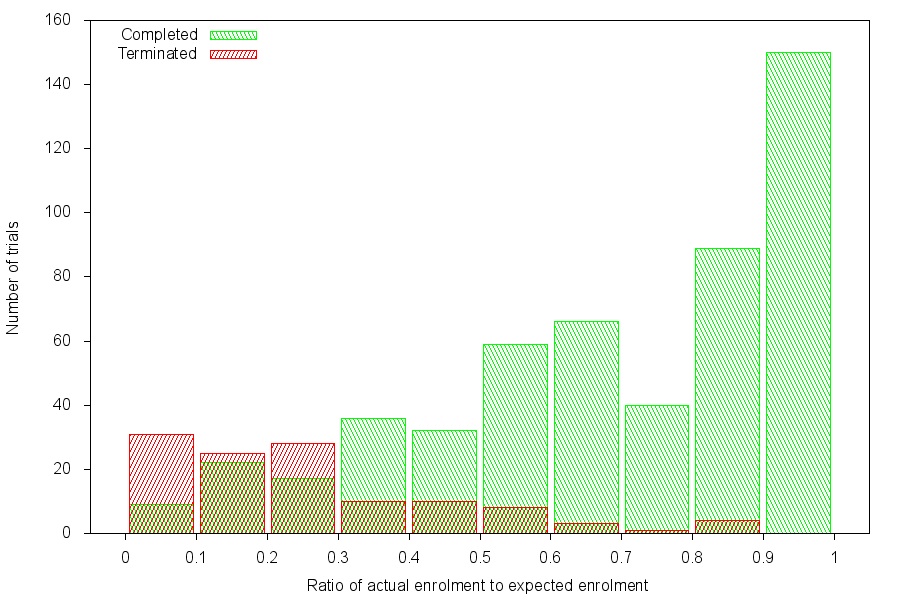
Ratio of actual enrolment to expected enrolment versus number of trials for trials that completed and trials that terminated due to poor accrual in 2011
The moral acceptability of a clinical trial is rooted in the risk and benefit for patients, as well as the ability of the trial to produce generalisable and useful scientific knowledge. The ability of a clinical trial to justify its claims to producing new knowledge depends in part on its ability to recruit patients to participate—the fewer the patients, the less confident we can be in the knowledge produced. So when trials have recruitment problems, those trials also have ethical problems.
In a recently published issue of Clinical Trials, my colleagues and I investigate the prevalence of poor trial accrual, the impact of accrual problems on study validity and their ethical implications.
We used the National Library of Medicine clinical trial registry to capture all initiated phase 2 and 3 intervention clinical trials that were registered as closed in 2011. We then determined the number that had been terminated due to unsuccessful accrual and the number that had closed after less than 85% of the target number of human subjects had been enrolled.
Of 2579 eligible trials, 481 (19%) either terminated for failed accrual or completed with less than 85% expected enrolment, seriously compromising their statistical power. A total of 48,027 patients had enrolled in trials closed in 2011 who were unable to answer the primary research question meaningfully.
Not only that, but we found that many trials that should have been terminated were pursued to completion, despite flagging rates of subject accrual, and the proportion of trials that completed was much higher than the proportion of trials that terminated, even at accrual levels as low as 30%. (See attached figure.)
The take-home message is that ethics bodies, investigators, and data monitoring committees should carefully scrutinize trial design, recruitment plans, and feasibility of achieving accrual targets when designing and reviewing trials, monitor accrual once initiated, and take corrective action when accrual is lagging.
@Manual{stream2014-615,
title = {Unsuccessful trial accrual and human subjects protections: An empirical analysis of recently closed trials},
journal = {STREAM research},
author = {Benjamin Gregory Carlisle},
address = {Montreal, Canada},
date = 2014,
month = nov,
day = 6,
url = {http://www.translationalethics.com/2014/11/06/trial-accrual-and-ethics/}
}
MLA
Benjamin Gregory Carlisle. "Unsuccessful trial accrual and human subjects protections: An empirical analysis of recently closed trials" Web blog post. STREAM research. 06 Nov 2014. Web. 26 Apr 2025. <http://www.translationalethics.com/2014/11/06/trial-accrual-and-ethics/>
APA
Benjamin Gregory Carlisle. (2014, Nov 06). Unsuccessful trial accrual and human subjects protections: An empirical analysis of recently closed trials [Web log post]. Retrieved from http://www.translationalethics.com/2014/11/06/trial-accrual-and-ethics/
As Jonathan is fond of saying: Drugs are poisons. It is only through an arduous process of testing and refinement that a drug is eventually transformed into a therapy. Much of this transformative work falls to the early phases of clinical testing. In early phase studies, researchers are looking to identify the optimal values for the various parameters that make up a medical intervention. These parameters are things like dose, schedule, mode of administration, co-interventions, and so on. Once these have been locked down, the “intervention ensemble” (as we call it) is ready for the second phase of testing, where its clinical utility is either confirmed or disconfirmed in randomized controlled trials.
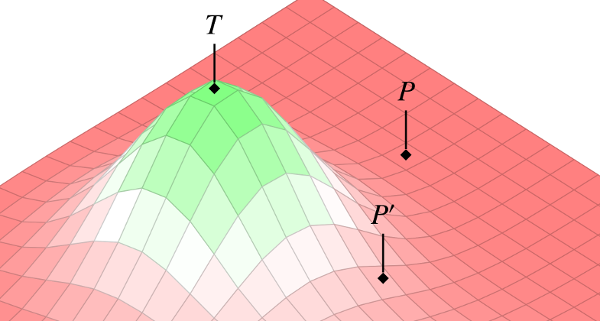
In our piece from this latest issue of the Kennedy Institute of Ethics Journal, Jonathan and I present a novel conceptual tool for thinking about the early phases of drug testing. As suggested in the image above, we represent this process as an exploration of a 3-dimensional “ensemble space.” Each x-y point on the landscape corresponds to some combination of parameters–a particular dose and delivery site, say. The z-axis is then the risk/benefit profile of that combination. This model allows us to re-frame the goal of early phase testing as an exploration of the intervention landscape–a systematic search through the space of possible parameters, looking for peaks that have promise of clinical utility.
We then go on to show how the concept of ensemble space can also be used to analyze the comparative advantages of alternative research strategies. For example, given that the landscape is initially unknown, where should researchers begin their search? Should they jump out into the deep end, to so speak, in the hopes of hitting the peak on the first try? Or should they proceed more cautiously–methodologically working their way out from the least-risky regions, mapping the overall landscape as they go?
I won’t give away the ending here, because you should go read the article! Although readers familiar with Jonathan’s and my work can probably infer which of those options we would support. (Hint: Early phase research must be justified on the basis of knowledge-value, not direct patient-subject benefit.)
@Manual{stream2014-567,
title = {The Landscape of Early Phase Research},
journal = {STREAM research},
author = {Spencer Phillips Hey},
address = {Montreal, Canada},
date = 2014,
month = jul,
day = 4,
url = {http://www.translationalethics.com/2014/07/04/the-landscape-of-early-phase-research/}
}
MLA
Spencer Phillips Hey. "The Landscape of Early Phase Research" Web blog post. STREAM research. 04 Jul 2014. Web. 26 Apr 2025. <http://www.translationalethics.com/2014/07/04/the-landscape-of-early-phase-research/>
APA
Spencer Phillips Hey. (2014, Jul 04). The Landscape of Early Phase Research [Web log post]. Retrieved from http://www.translationalethics.com/2014/07/04/the-landscape-of-early-phase-research/